Traditional total hip replacement surgery involves removing the damaged portions of the hip joint and replacing both the ball (femoral head) and the socket (acetabulum) with artificial components. This method has been performed successfully for decades and is considered a reliable treatment for advanced hip arthritis or other severe joint damage.
The prosthetic components are typically made from metal, ceramic, or high-grade plastic materials designed to mimic the natural movement of the hip and reduce joint friction. Traditional total hip replacement can significantly relieve pain, restore mobility, and improve quality of life when other treatments have not been effective.

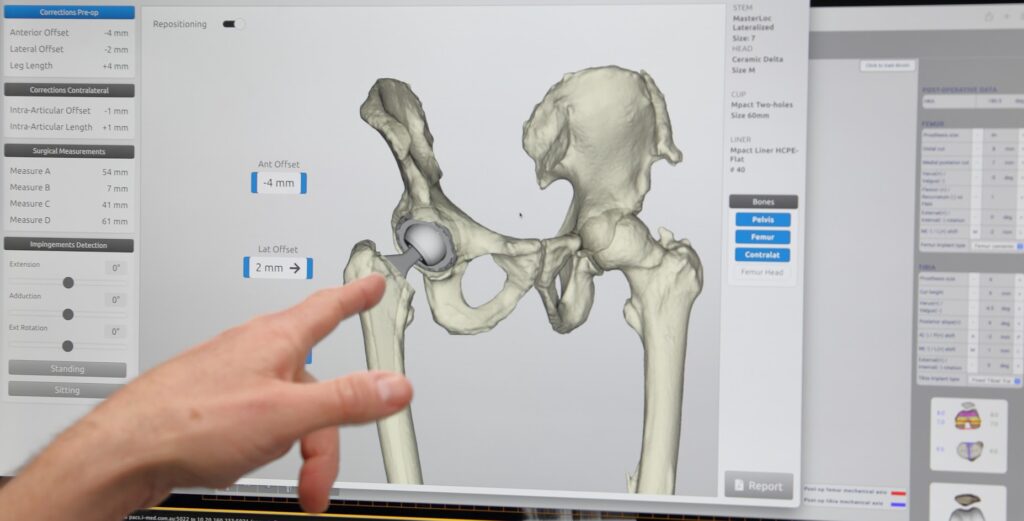
Minimally invasive total hip replacement is a surgical technique that aims to reduce soft tissue disruption while achieving the same goals as a traditional total hip replacement. The implants used are the same, and this approach may be applied through various surgical entry points, depending on your individual condition and the surgeon’s recommendation.
The key difference lies in how the procedure is performed. Minimally invasive methods typically involve smaller incisions and careful handling of muscles and soft tissues, which may support a smoother recovery in some patients.
Potential features of a minimally invasive hip replacement may include:
Smaller incisions: The surgical cut is often shorter, generally around 7–10 cm, compared to the longer incisions used in traditional techniques.
Reduced muscle disruption: The approach generally involves gently moving muscles aside rather than cutting through them, which may help reduce post-operative discomfort.
Quicker recovery: Some patients may experience a shorter hospital stay and a faster return to daily activities, though recovery times can vary depending on individual factors.

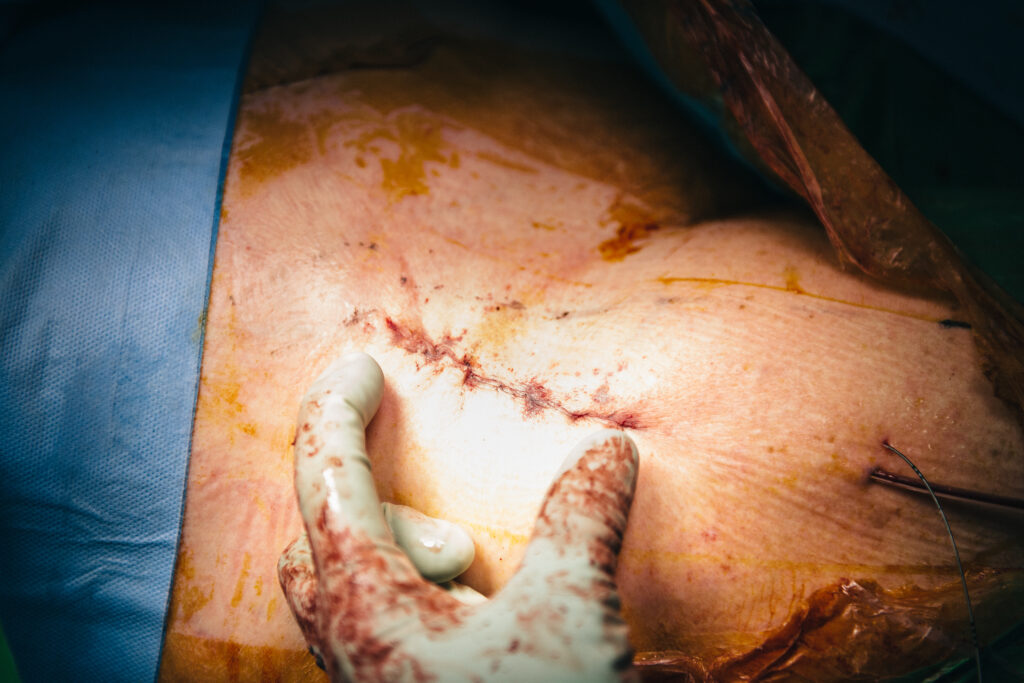
The Bikini Incision total hip replacement is a specific type of minimally invasive surgery. It is named for the location and shape of the incision, which follows the natural lines of the groin, similar to the line of a bikini bottom.
The bikini incision total hip replacement approach may offer several advantages:
- Cosmetic Benefit: The incision is less noticeable as it follows the natural skin crease, making the scar less visible.
- Muscle Sparing: This technique avoids cutting through major muscles, potentially leading to a quicker recovery and less postoperative pain.
- Reduced Risk of Dislocation: By preserving muscle and tendon structures around the hip, the stability of the joint is maintained, reducing the risk of hip dislocation post-surgery.

The anterolateral approach to hip replacement involves an incision positioned at the front and side of the hip. This surgical technique is designed to offer a balance between preserving muscle tissue and providing the surgeon with clear visibility of the hip joint.
Key features of the anterolateral approach:
Incision placement: The incision is typically made along the front and side of the hip, approximately 10–15 cm in length. This location allows access to the joint while aiming to minimise disturbance to major nerves and blood vessels.
Muscle preservation: Instead of cutting through major hip muscles, this approach works between the fibres of the gluteus medius and minimus. This may help retain muscle strength and support post-operative recovery.
Potential benefits:
By sparing key muscles around the hip, the anterolateral approach may offer improved joint stability, which may help reduce the risk of hip dislocation following surgery.
Considerations:
Although this technique avoids cutting the gluteus medius, it may involve significant traction (pulling) on surrounding muscles such as the gluteus medius and tensor fascia lata (TFL), as well as potential strain on the superior gluteal nerve. For this reason, while the anterolateral approach is used in some European centres, it is less commonly performed in Australia, the United Kingdom, and the United States due to the risk of muscle or nerve irritation.

The lateral approach to total hip replacement involves accessing the joint from the side of the hip. This technique is one of several established surgical approaches used to treat hip arthritis and other degenerative joint conditions.
Key features of the lateral approach:
Incision placement: The incision is made along the outer (lateral) side of the hip, allowing the surgeon a direct view of the joint.
Muscle involvement: To reach the joint, parts of the hip abductor muscles—specifically the gluteus medius and minimus—are partially detached during surgery. These are carefully repaired and reattached once the prosthetic components are in place.
Potential advantages:
This approach allows for excellent visibility of the hip joint and may be associated with a lower risk of dislocation compared to the posterior approach. It is a widely used technique with a long track record in hip replacement surgery.
Things to consider:
Due to the involvement of the hip abductor muscles, some patients may experience a temporary limp or weakness after surgery. A structured physiotherapy program is often needed to support healing and help restore full function over time.
The posterior approach is one of the most commonly performed techniques for hip replacement surgery. This method involves making an incision at the back of the hip to access the joint and replace the damaged bone and cartilage with prosthetic components.
What to expect with the posterior approach
Incision location: The surgical incision is made along the side and back (posterior) of the hip, providing direct access to the joint.
Muscle technique: The gluteus maximus muscle is gently split, and some of the small external rotator muscles are temporarily released and later repaired to gain access to the hip joint.
Surgical advantages: This approach offers excellent visibility of the hip, allowing for precise placement of implants. It is suitable for a wide range of patients and has a long track record of successful outcomes.
Things to consider
While this technique is widely used, there may be a slightly increased risk of dislocation in the early stages after surgery. Patients are typically advised to follow specific movement precautions during the initial recovery period to support joint stability.

The SuperPATH approach (short for superior percutaneously assisted total hip replacement) is a modern variation of the posterior approach. Sometimes called a “mini-posterior” technique, it is designed to be less invasive than traditional hip replacement surgery by using smaller incisions and minimising disruption to muscles and tendons around the hip.
What makes the SuperPATH approach different?
Minimally invasive technique: The procedure is performed through a small posterior incision, typically avoiding the need to cut major muscles.
Muscle preservation: By working between natural muscle planes and preserving tendons, this approach aims to support post-operative stability and recovery.
Potential benefits: Patients may experience reduced pain, shorter hospital stays, faster rehabilitation, and a quicker return to everyday activities. The technique may also result in a smaller scar and a lower risk of dislocation due to better preservation of soft tissues.